Shoeing for Palmar Hoof Pain
Introduction
|
Palmar hoof pain (PHP) is usually defined as a positive reaction (absence or decrease of lameness) after a distal palmar digital nerve block ( DPDN block near the margin of the ungular cartilages). Although sometimes defined as a “heel block”, it anesthetizes the DIP joint, the entire sole, the distal phalanx (PIII) and the navicular apparatus ( 1/ Schumacher 2006) |
Besides podotrocleosis, which in itself is a condition which encompasses more than just “naviculitis “or “navicular syndrome “, PHP may therefore be due to:
- Heel or solar bruises and / or abscesses.
- Severe thrush or canker.
- Trauma to the bulbs ( over reaching injuries ).
- Osteitis of P III.
- (wing) fractures of P III.
- Quarter cracks.
- Quittor.
- Artrosis-arthritis of the DIP joint.
|
The last is not always easy to differentiate from podotrocleosis) as DIP joint anesthesia ( especially when more than 6 ml of local anesthetic is used ), might, by distending the palmar pouches, anesthetizes the DPD nerves.( 1/ Schumacher 2006).
|
Clinical examination
|
Careful clinical examination, including inspection, palpation, pulse taking and judicious use of hoof testers ( before anesthesia of course ), remains the most valuable tool in differentiating among the different conditions mentioned above. This examination requires patience and more clinical skills than is often assumed, but can , together with a good history work up, often save a lot of frustration.
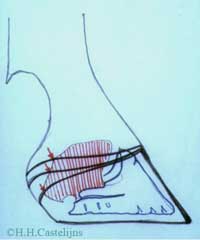
An especially valuable clinical test is the digital extension / elevation test. Traditionally done with a board, this test evaluates the horse’s tolerance to dorsal extension, ( 2/Desbrosse, 2002).[ fig.1.a,b,c,].
|
|
|
|
Fig. 1 a-b-c:
Use of a graduated digital extension device.
|
|
A graduated Digital Extension Device ( DED) has been developed by the author which , besides measuring the exact degrees of tolerance to the dorsal extension of each forelimb, also permits evaluation and measurement of the tolerance to lateral and medial elevation of the foot, which causes collateromotion of the DIP joint ( 3/ Chateau et al, 2002).
Tolerance to dorsal extension is variable for each limb, depending on conformation, and can vary in sound horses from around 30° ( some quarter horses with straight short pasterns and “ tighter “ deep digital flexor tendons (DDFTs), to over 45° ( e.g. some thorough bred horses with long oblique pasterns ,and lax DDFTs).
Sound horses tolerate lateral and medial elevations of the foot till the opposite side of the foot lifts off the surface of the DED. The degree of elevation at which this occurs , is much more standardized across breed- and conformation types, than dorsal elevation; typically being 19° of lateral elevation and 20-21° of medial elevation. Differences between lateral and medial degrees, are probably due to the fact that the test is performed with the opposite limb held off the ground, whereby the horse places the weight bearing , and tested , limb , closer to the midline of its body. |
Intolerance to dorsal extension may indicate :
- Podotrocleosis, including bursitis, impar ligament desmitis, distal DDF tendonitis and desmitis of the collateral ligaments of the distal sesamoid.
- Proximal DDF tendonitis.
- Inferior check ligament desmitis.
- Dorsal laminar inflammation.
|
Intolerance to lateral or medial elevation may indicate:
- DIP, PIP or MC Phalangeal collateral ligament desmitis ( on the opposite side of the elevation)
- Laterally or medially located subcondral bone lesions of the digital joints ( on the ipsilateral side of elevation).
- Lateral or medial suspensory ligament branch desmitis ( opposite side ).
- Arthrosis of digital joints with lateral or medial bone spur formation ( ipsilateral side , generally).
- Distal DDF tendonitis located in the lateral or medial lobes of the tendon, (opposite side).
- P III fractures ( wing, ipsilateral side).
- Trimming mistakes are characterized by reduced elevation values on one side, accompanied by increased elevation values on the opposite side of the foot (trim more on the side of reduced elevation values).
|
Finally, there are conditions which might reduce tolerance to extension in a combination of directions: dorsal and lateral, dorsal and medial, lateral and medial, all three.
|
Diagnostic Imaging
|
In recent years diagnostic imaging has made great strides, as first ultrasound and then MRI and CAT have allowed for much more detail when “looking” into the foot. High quality, ( digital) X rays, including the use of contrast material, have also progressed, but the great difference is certainly the ability to better detect soft tissue injuries, which generally precede bony lesions.[ fig.2]
|
|
Fig 2:
When radiological signs appear, soft tissue lesions can already be very severe.
Photo courtesy Michael Savoldi.
|
|
Better diagnostics though, also means finding more lesions, often in different , even adjacent structures, each of which theoretically requires different biomechanical solutions ( read shoeing strategies ) . This is another point which indicates the importance of a good, clinical work up; e.g. if a lesion in the distal DDFT, adjacent to a lesion in the straight distal sesamoidean ligament is detected, it is necessary to find out if the horse resents dorsal digital extension more than fetlock extension, before prescribing therapeutic shoeing. [ fig.3.a,b.].
|
Therapeutic shoeing techniques.
|
The following elements should be taken into account when considering shoeing prescriptions:
- Type of lesion, clinical signs.
- Type of work-performance expected from the horse.
- Surface the horse works on.
|
The last element is of paramount importance, because a lot of shoeing techniques which are based on changing around the ground wearing surface of the shoe, only work on penetrable ground. As far as the type of work goes, some disciplines require an enormous amount of work on ( tight) circles others do not ( e.g. standard bred racing).
Some lesions hold out hope for eventual healing ( e.g. some soft tissue injuries ), and the therapeutic shoeing will only be temporary; other lesions are permanent ( e.g. ring bone),and therapeutic shoeing techniques will be necessary for the rest of the horse’s (working) life.
General objectives of therapeutic shoeing is to spare painful structures, but this can only be done by loading other structures more: e.g.: a reverse shoe on soft ground relieves the DDFT, but loads the superficial DFT and the suspensory ligament ( S:L.) more.
|
Table 1 : Illustrates therapeutic shoeing techniques for Palmar Hoof Pain conditions excluding DIP-PIP artrosis and podotrocleosis |
Condition |
Ground surface |
(Treatment) trimming, shoeing techniques- Other comments |
a)heel or solar bruises/abscesses |
Compact /deep |
1)drainage, preferably through the hoof wall (not through the sole). Local disinfection animal lintex |
2) Shoes which offer protection to the seat of corn, to the sole[ fig.4 ] ; hospital plates, open up pad , which can keep bandaging or packing in. |
b) thrush or canker |
Compact/deep |
1) surgical debridement |
2) hospital plate |
3) topical application of 50 /50 picryc acid and salicylic acid in powder form every 2/3 days postop. |
c/ traumas to the bulb |
Copact/deep
( often on deep ground) |
Topical treatment |
Over reach boots after healing, setting back the hind shoes, facilitating quicker dorsal break over on the front shoes ( rolled, set back front shoes) slightly lowering , feathering the heels on the front hooves, shoes. |
d) osteitis of P III |
Compact/deep
(More problems on hard ground ) |
1.dorsal edge of P III ( responds to DPDN block) increase sole depth under the tip of
P III, ( Rim) pads, glue on shoes, medium hard sole support packing under the palmar part of the hoof.
2. Palmar processes ( negative palmar angle of P III), increase palmar sole depth, frog support pads ( e.g. P.M: pads ) soft silicone or polyurethane packing. Onion shoes with high quality leather pads or Luwex Senior pads. Do not raise heels. Note : In case of ( post neuroctomy) DDFT laceration: desmotomy of the extensor branches of the fetlock suspensory apparatus. (5 Leveillard ). [ fig.5]. |
e) (wing ) fractures of
P III |
Stall rest recommended
Rehab. on soft ground |
- Sagittal fractures : four clipped shoe ( two clips ahead of the widest part of the hoof, two clips just behind the widest part ) beveled ground surface of the shoe, negative pressure heart bar, that is with space between frog plate and frog. [fig.6 a,b.]
- Wing fractures: idem with three clips ( quarter clips plus one clip at the heel of the fractured palmar process).
|
f) quarter cracks ( q.c.) |
Compact/deep
( worse on compact surface) |
1-Spontaneous, descending , painful q.c.’s are caused by ipsilateral ungular, Cartilage entrapment by a shunted –up heel wall. Heel wall should be lowered , to obtain at least 15 mm of free ungular cartilage margin above the hoof wall. [ fig.a,b ] This is best done with a double trim method whereby after the initial trim of the hoof, a second trim on the side of the q.c. is performed , which goes from 0 at the ipsilateral toe to 6-8- mm at the ipsilateral heel in a straight line.
2-Debridement , medication, drainage and fixation of the crack.
3-Frog-support. COPPSC ( « Mercedes shoes”). [ fig.8a, b]
Do not raise heels! ( 6 /Castelijns) |
g) Quittor |
Compact/deep |
Surgical debridement, regional A.B. perfusion, bar shoes, bandaging. |
|
Table 2 : Illustrates therapeutic shoeing techniques for DIP-PIP artrosis and for podotrocleosis
|
Condition: DIP, PIP artrosis and / or podotrocleosis, |
Intolerance to: |
Works on surface |
Shoeing , trimming techniques |
e.g. single collateral ligament lesion , single lobe of distal DDFT.., single collateral ligament of Nav. |
Lateral or median elevation |
deep |
Narrow web shoe, beveled ground surface on the side of intolerance , wider ground surface on the opposite side, short hooves , short shoeing intervals. [fig.9] |
compact |
- flexible shoes ( e.g. Flaps, easy walker) .[ fig.10].
- strongly beveled ground surface ( outside rim) on the side of intolerance.
- Rockered ipsilateral toe shoe ( “ French rockered toe “).
- Full rolling motion shoes, slightly displaced towards the opposite side of the intolerance. Note:Short intervals do not leave heels too long / high, specially in the case of dorsal entheseophytes.
|
e.g. DIP artrosis artritis |
Lateral and medial |
deep |
- short, barefoot trim, well rounded borders not too much heel.
- Flexible shoes, short shoeing intervals
- Half round section shoes, tightly fit ( e.g. classic roller or eventer). [ fig.11].
|
compact |
- “French rockered toe” ( rocker goes from quarter over the toe to opposite quarter; heels stay flat.
- Half round section shoes.
- Full rolling motion shoes ( e.g. “rock n roll”, PG shoes ).[fig.12 a,b.]
Note: consider shock absorption ( aluminum, pads), keep shoeing intervals short , do not set the shoes too wide . |
e.g. NAV. Bursitis
Distal DDF tendonitis impar lig. Desmitis. |
Dorsal extension |
deep |
- rolled-rockered - set back- toe shoes.
- the same plus egg bar.
- Reverse shoeing. [fig.13].
|
compact |
- rolled-rockered toe.
- Blunt- set back toe, e.g. NBS or Sagittal.[fig.14,a,b]
- Aluminum square toed ( wear is faster in the toe between shoeing intervals).
- Shock absorbing pads, mild frog support pads ( test for sensibility of the frog area).
- Full rolling motion shoe’s with the ground area at the toe strongly beveled; the higher total thickness of the shoe permits an extreme rolled toe .
|
e.g. DIP arthrosis and podotrocleosis |
Dorsal extension and lateral and medial elevation. |
deep |
- Set back shoe (blunt toe) with beveled ground edges and egg bar.
- Palmar frog and sole support. ( less heel penetration).
- Full rolling motion shoe with heel bar. [fig.15]
|
compact |
- Full rolling motion shoe, with small central base, well set back.
- Shock absorbing pad if sensitive to hammer blows to the shoe, short shoeing intervals.
|
|
|
Fig. 3a-b:
Adjacent lesions of the DDFT and the straight distal sesamoidal ligament;
unloading one will overload the other
|
|
|
Fig. 4:
Sole abscesses need protection after drainage
|
|
Fig 5:
Post neurectomy DDFT laceration
|
|
|
Fig 6a-b:
Sagittal fracture of PIII; clip shoe with negative pressure herat bar
|
|
|
|
Fig 7a-b:
Ungular cartilage palpation, measurement and relation to the hoof capsule
|
|
|
|
Fig 8a-b:
Mercedes shoe and polyurethane sole support
|
|
|
Fig 9:
Wide web branch shoe, the narrow, penetrating branch should be placed on the side of the foot which shows intolerance to elevation
|
|
Fig 10:
Flexible easy walker shoe
|
|
Fig 11:
Half round section-heart bar shoe: lots of break over, less heel sinking
|
|
|
Fig 12a-b:
Full rolling motion shoes (Rock n' Roll shoe and PG shoe)
|
|
|
Fig 13:
Reverse shoe, dorsal break over, less heel sinking
|
|
|
Fig 14a-b:
Sagittal shoe, blunt toe, rounded edges, bar support
|
|
|
Fig 15:
Full rolling motion shoe with heel bar
|
|
|
Fig 16a-b:
When raising the heels with wedges, the coronary band is pushed upwards
|
|
|
Fig 17:
Myron McLane pad, note the heel wedge and the flexible frog pad
|
|
|