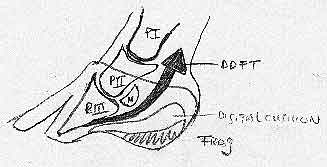
Hoof care for laminitis and founderAbbreviations and notes to the reader: PIII: the distal phalanx 1. IntroductionLaminitis (the inflammation of the sensitive laminae connecting the distal phalanx to the hoofwall) is a medical emergency and its treatment aims at preventing founder (which can be the consequence of the former and indicates loss of the normal pedal bone - hoof capsule relationship). For an excellent - medical emergency treatment overview of acute laminitis see “Medical and Surgical Treatment of Acute Laminitis in Horses” by F.Desbrosse, in European Farriers Journal nr. 71, page 18-43. Part of this emergency treatment consist of relieving the weight bearing function of the (dorsal) hoofwall which sustains PIII through the affected laminae. This can be obtained by transferring weight-bearing function to the palmar aspects of the sole, including the bars, and to the entire frog, which are not affected by the laminar inflammation. One easy and quick way of doing this is by applying a foot cast with extra support below the palmar structures.
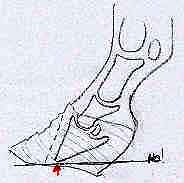
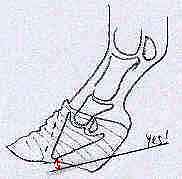
2. Shoeing for founder:Once there is downwards displacement of PIII relative to the hoof capsule - rotation (dorsal laminae detached) and / or sinking (lateral and medial laminae are also detached) - therapeutic shoeing should have the following aims: a) Protect and re-establish “sole depth”; that is about 17-20 mm of sole below the tip of PIII. Permanent damage to a laminitic patient comes from loss in this area of PIII. This bone loss is a consequence of chronic inflammation (osteitis) due to the pressure of the tip of PIII on the anterior part of the (life) sole. The corium of the sole is compressed between PIII from above and the flattened horny sole from below. Sole perforation and abscesses (solar corium necrosis) are common consequences and need treatment possibilities and therefore access. This means that the sole in front of the frog should not be covered permanently and should not bear weight or even contact with the shoe pad or the ground. b) Unload the wall (and therefore the affected laminae) by transferring weight bearing to the palmar sole - bars and frog. Diminished weight bearing by the affected laminae reduces inflammation and pain and facilitates healing. c) Promote normal hoof capsule - PIII alignment by trimming back the dorsal wall till it is parallel to the dorsal aspect of PIII but also by trimming the heels if the angle of PIII with the ground, as seen on a correctly performed Latero - Medial radiographic image, is more than 3°-7° degrees. This angle is called the palmar angle of PIII and is increased in the case of palmar - rotation of PIII under the influence of DDFT pull. Note: What has been described here addresses what some authors have called capsular and phalangeal rotation. d) Release DDFT pull on PIII. The horse does this through increased heel growth, the farrier can do this through raised heel shoeing and / or by bringing dorsal break-over back (e.g. open toe shoeing), the Veterinarian can do this through DDFT tenotomy. Permanent shortening (contracture) of the DDFT tendon - muscle and inferior check ligament complex is another long-term damage (together with bone loss) which can keep a foundered horse from full recovery. The longer a horse has an increased palmar angle of PIII to the ground the easier it is for DDFT contracture to take place. Chronic founder horses which "walk" toe first instead of heel first are signalling their flexor contraction. It should be noted that it is not the same to have excessively long (tall) heels (increased palmar angle between PIII and the hoof) and raised heel shoes (increased palmar angle between PIII and the ground but not with the hoof). Bringing back dorsal break-over radically (which in horses with palmar rotation is often further forward then normal to begin with) releases DDFT pull in the cranial stride phase, when it is strongest. When trimming the heels the sole depth below the tip of PIII should be respected, in other words do not trim from the toe to the heels, but only the heels! (Fig. 2)
e) Decompression of the coronary band.
(Dorsal) Hoof wall growth is stunted because of the mechanical compression (less blood flow) of the coronary band and misdirected because of the bent papillae. In palpating the coronary band one notices a depression just above the hairline (proximal border of the hoof capsule) radiologically the distance between the (marked) top of the dorsal wall and the extensor process of PIII is increased. On a latero - medial venogram the shape of the dorsal coronary band looks like a “flame” instead of a “circle” and is darker (less blood) then normal. (Fig. 4)
Decompression (and instant lowering) of the coronary band can be achieved by hoof
f) Reduce Pain
g) Prevent abscesses: A lose laminar bond, necrotic tissue, a widened white line, all favour the formation of abscesses; to combat these there should be access to necrotic tissues through partial hoofwall resection, subcoronary grooves and easily removable shoes or pads which permit local treatment. 3. The Castelijns - Rosello method:The veterinary surgeon Gaspar Castelijns together with the farrier Ricardo Rosello pioneered a shoeing system which addresses the aims mentioned before very effectively. After trimming the dorsal hoof wall parallel to PIII and at an appropriate thickness and establishing a close to normal palmar angle by trimming back the heels, a Dallmer Cuff is glued on the previously cleaned and dried remaining hoof wall with fast setting polyurethane's or acrylics.
By forging down the front part of the shoe and by screwing it on further back, dorsal break over is moved caudally (less DDFT pull). (Fig.8) Because of the rolling motion shoe type design, not only dorsal but also latero medial break over is facilitated, which makes turning, with its asymmetrical tensions on the hoof capsule - PIII bond, much less pain full for the patient. (Fig.9)
The 7 mm thickness of the bottom of the glue on cuff gives welcome and extra sole depth, prolapsed soles can be inspected and treated with disinfectants by simply unscrewing the full rolling motion shoe which trough its closed design offers full protection to the sole. The cuff can be opened at the toe, to gain access to dorsal wall or sole cavities and is compatible with subcoronary grooving. (Fig.10) - (Fig.11)
The gluing on is atraumatic and with the use of Superfast (winter) or Adhere (summer) so fast that it can almost always be done without regional anaesthesia of the opposite limb (do the most pain full limb first, place the other on a block of Styrofoam). Once healthier hoof wall has grown down, at least at the heels, and a good sole depth has been obtained the Rockn'Roll can be nailed on the hoof directly, always in combination with condensation silicone as palmar support. This same method is very effective in mild cases of founder or at the beginning of laminitis. (Fig.12)
There are some extreme cases where sloughing of the entire hoof capsule is inevitable, facilitating the removal of the detached hoof capsule seems to bring relieve but nothing to nail or glue on to! Deep bedding, good bandaging and nursing can tie these patients over till they have grown a new hoof capsule back, a process which goes much quicker then one would expect. (Fig.13) - (Fig.14)
The real unretrievable loss in founder cases is bone loss from PIII, the hoof capsule grows back as long as the coronary band is relieved from mechanical pressure, by the upwardly displaced hoof capsule and is not damaged by compressive bandaging or casting. |












Hans Castelijns
D.V.M - Certified Farrier